ENT (Ear Nose Throat)
ENT Department (Otorhinolaryngology)
The ENT Department is a specialized center of excellence dedicated to the intricate structures of the head and neck. Because this region houses the vital organs for hearing, balance, smell, and speech, the department utilizes microscopic precision and advanced endoscopic technology. For international patients, this facility represents a "Center for the Senses," where delicate surgeries are performed with sub-millimeter accuracy to restore communication and quality of life.
Specialized Sub-Specialty Teams
The complexity of the head and neck requires a team of highly focused experts, each mastering a specific sensory or anatomical domain:
Otologists and Neurotologists: Specialists in hearing and balance who perform microsurgeries like Cochlear Implants and eardrum reconstructions.
Rhinologists: Experts in the nasal passages and sinuses who utilize advanced "Skull Base" surgery to treat chronic sinusitis and nasal polyps.
Laryngologists: Dedicated voice and swallowing specialists who treat professional speakers and singers for vocal cord disorders.
Head & Neck Surgeons: A specialized oncology and surgical team focused on the management of thyroid, salivary gland, and throat tumors.
Pediatric ENT Experts: Specialists who provide gentle, sized-down care for children facing issues like tonsillitis or "glue ear."
Audiology & Speech Pathologists: Professionals who provide diagnostic hearing tests, fit advanced hearing aids, and lead speech rehabilitation.
Advanced Technology and "Keyhole" Precision
The department is heavily equipped with high-definition visualization tools to navigate the narrow corridors of the ear, nose, and throat:
High-Powered Otomicroscopes: Advanced floor-mounted microscopes used to visualize the tiny, microscopic bones of the middle ear during surgery.
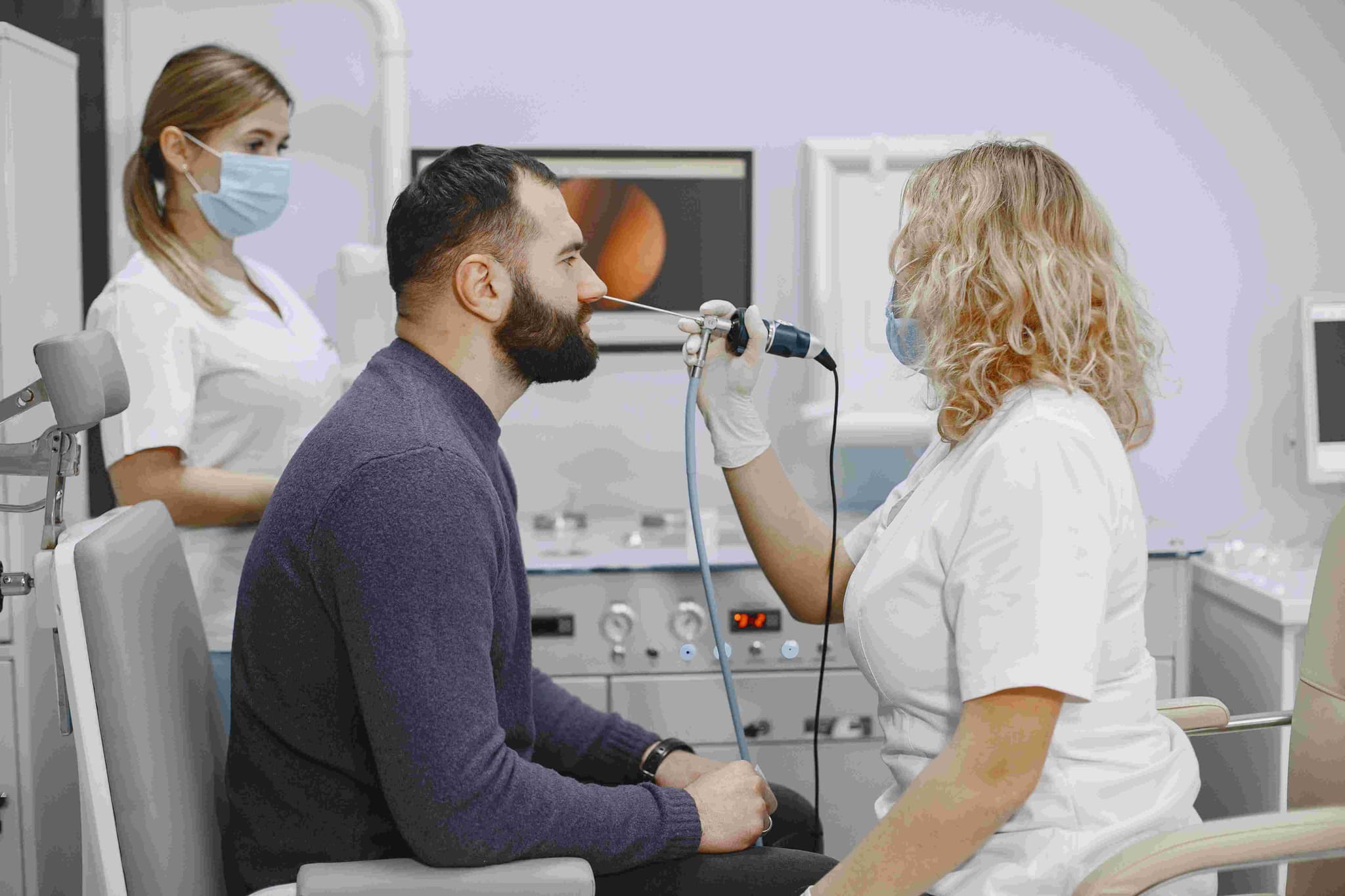
Flexible Fiber-Optic Endoscopy: Ultra-thin "noodle" cameras that allow for a live, awake view of the vocal cords and deep sinus openings.
Microdebrider & Laser Technology: High-speed, precision tools that allow for "bloodless" tissue removal while protecting healthy surrounding structures.
Intraoperative Nerve Monitoring: A critical safety system that tracks the facial nerve during surgery, ensuring the preservation of facial expressions and speech.
Vestibular Testing (VNG): Advanced diagnostic goggles that track eye movements to pinpoint the exact cause of vertigo and balance disorders.
Comprehensive Diagnostic and Wellness Facilities
To ensure a total recovery, the department houses specialized units for testing and therapy:
The Vertigo & Balance Clinic: A dedicated space for evaluating inner ear function and providing vestibular rehabilitation.
The Speech & Voice Lab: A computer-integrated environment used to analyze vocal pitch and intensity for post-surgical recovery.
Modern Allergy Wing: On-site "Skin Prick" and blood testing to identify environmental triggers for chronic sinus inflammation.
Sleep & Snoring Lab: Specialized diagnostic suites for identifying airway collapse during sleep apnea through Sleep Endoscopy (DISE).
International Patient Support: A dedicated office to assist global patients with surgical planning, hearing aid mapping, and post-operative follow-up.
A Commitment to Sensory Restoration
The department focuses on minimally invasive techniques to ensure patients return to their daily lives as quickly as possible:
Scar-Free Surgery: Most sinus and voice procedures are performed through natural openings, leaving no external marks.
Rapid Recovery Protocols: Utilizing laser and coblation technology to minimize post-operative pain and promote faster healing of delicate tissues.
Holistic Communication Care: Combining surgical success with long-term speech and hearing adaptation for a complete return to social and professional life.